

In previous articles, we’ve:
- described oral language and language therapy;
- explained that oral language includes oral language comprehension; and
- outlined how oral language comprehension skills affect reading comprehension.
But what do we mean when we use the term ‘oral language comprehension’?
This is a big topic. We’ll break it down, starting with the name.
Oral language comprehension is sometimes called:
- “language comprehension”;
- “receptive language”; or
- “listening comprehension”.
All these terms mean the same thing. But, whatever you call it, oral language comprehension is:
- controversial as a standalone idea;
- hard to define;
- important for people of all ages and abilities;
- assessed by speech-language pathologists, especially when we want to know whether someone has a developmental language disorder (DLD) or other language problem;
- tricky to measure; and
- tough to treat if there is a problem.
1. Is oral language comprehension even a real thing?
Some researchers think there is not much point talking about oral language comprehension in isolation from the rest of language. Language is a complex system – all the parts affect each other, sometimes in unpredictable ways.
We think they’re right. But, in the clinic, when we come across someone struggling to participate fully at school, work, or in life, we want to check whether they are having problems understanding language.
2. So what is oral language comprehension?
We use four main frameworks to think about language comprehension:
Model 1: A general framework
Oral language comprehension is a “process during which information is received and then transformed into different types of representations until the meaning is worked out using your existing general knowledge” (e.g. Bishop, 1997; Acosta-Rodriguez et al., 2022 – see full citation below).
What on earth does this mean?
Let me explain in plain English with concrete examples:
- In our lives, we hear all sorts of information, including:
- spoken language (e.g., from family members, friends, teachers, colleagues, and others, as well as recorded spoken words on the radio, TV, and Internet); and
- non-language sounds (e.g. sirens, dogs barking, and construction noise).
- Oral language comprehension is – you guessed it – about spoken language, not about how we interpret other types of noise.*
- Language-based information includes:
- words;
- sentences; and
- discourse.
- ‘Discourse’ means spoken or written language used in a particular place and time. For oral language, it includes spoken language in conversations with other people, e.g. during play, or in meetings at work, as well when listening to others speak at length, e.g. when telling us stories or explaining how things work.
- When we hear spoken language, we turn it into different types of representations in our brains. This is probably best explained with an example:
Imagine you hear a loud knock on your door at 11.30pm on a Saturday night in the middle of winter. Groggily, you open the door and find a police officer pointing up urgently at your front window. She says: “The steel bars are broken”.
- You would hear the police officer, and transform what she said into different kinds of representations in your brain:
- speech sound representations (phonemes), e.g. the sounds /b/, /a/ /z/;
- word representations (lexemes), e.g., the word “bars”;
- representations of meaningful word parts (morphemes), e.g., recognising the regular plural -s after the noun “bar”, means there is more than one bar;
- sentence grammar representations (syntax), e.g., recognising:
- a subject-verb-complement sentence, with “bars” as the subject; and
- the different parts of speech used in the sentence: definite article (‘the’) + adjective (‘steel’) + noun (‘bars’) + present tense verb (‘are’) + adjective (‘broken’);
- knowledge of word-meanings and relationships between word (semantics), e.g. knowing that the “bars” being referred to are steel rods, and not the type of bars young adults frequent on Saturday nights; and
- pragmatic knowledge, e.g., that – taken together – the spoken sentence and gestures of the police officer, the social context of a police officer coming to your house late at night during winter to speak with you, and your existing knowledge of the world (including about police, and the function of bars on windows), suggest that the broken steel bars are something you should be concerned about as a priority.
Model 2: Referential and Inferential Language Comprehension
When you step up from words and sentences to discourse (e.g. conversations and stories), you need inferential comprehension. As we explain here in the context of reading, inferencing is the ability to combine:
- what is being said; with
- what we already know,
to understand the spoken language. When talking about spoken discourse, some researchers describe oral language comprehension as a system with two levels:
(i) Referential comprehension
When you hear a story, you process the exact words and sentences, including the vocabulary and the grammar used, to understand what is being said. This is sometimes described as a ‘surface level’ or ‘lower level’ task (Dijk & Kintsch, 1983), and it includes two components:
- Word comprehension links the sequence of sounds within a given word with your mental dictionary of words. It includes knowledge of subword units like phonemes, syllables and morphemes).
- Sentence comprehension involves using your knowledge of words and syntax together to form more complex units of meaning.
(ii) Inferential comprehension
When you hear a story, you are not trying to memorise the words and sentences. Instead, you seek to construct a mental model or situation model of the characters, events, objects, places and actions described, and the relations among them. This is sometimes described as a ‘higher level’ task (Tapiero, 2007; Johnson-Laird, 1983).
You must integrate the information you hear into a coherent structure that unites the different statements, and incorporate them into your general knowledge. In doing this, the main types of inferences to understand the language you hear are:
- local inferences, also known as “gap-filling inferences”; and
- global inferences, also known as “text-connection” or “bridging” inferences (e.g. Graesser et al., 1994; Cain & Oakhill, 1999).
We explain local and global inferences in more detail, with examples, here. In essence, you connect what you hear, the context in which you hear it, and your general knowledge of the world to make sense of the language you hear.
Model 3: Oral language comprehension as a component of the Simple View of Reading
Language comprehension is one of two main components of the Simple View of Reading. We’ve written about this useful model extensively, including here and here and here and, most recently, here. (We’ve fans!)
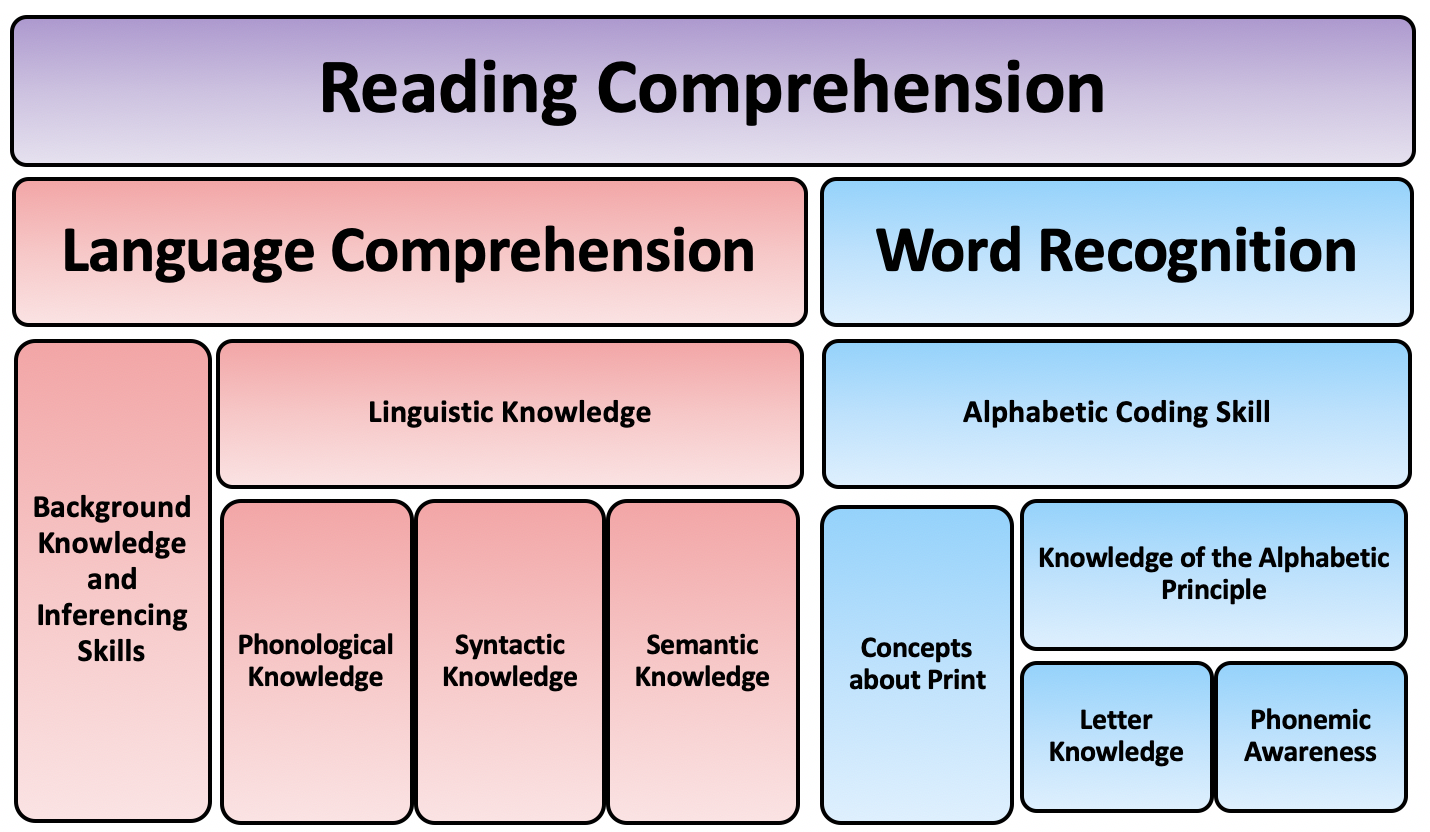
The cognitive foundations framework. Source: Hoover and Tunmer (2019).
The latest iteration of the model – called the Cognitive Foundations Framework – subdivides language comprehension into the following components:
- Phonological knowledge;
- Syntactic knowledge;
- Semantic knowledge, including vocabulary and semantics, and higher level language skills like metaphors, idioms and analogies;
- Background knowledge; and
- Inferencing skills.
We use this model most frequently with students with reading difficulties, including reading comprehension difficulties. In practice, this model is consistent with the general and two-level models outlined above. But the Simple View of Reading can help us to think clearly about priorities, and the best sequence of therapies to help beginning readers, as well as students with both language and reading difficulties.
Model 4: Capacities-focused vs. processing models
Not all health and education professionals agree on the core underlying processes and capacities that affect or contribute to oral language comprehension. As we’ve outlined here (again in the context of reading):
- Capacities are about language abilities – the language that people can understand.
- Processes are cognitive operations underpinning language, including things like the mechanisms for converting speech sounds that reach the ear into phonological representations, and then into links to the brain’s internal dictionary of words.
This all sounds a bit theoretical. But it can have a big impact on how you think about, assess, and support someone with oral language problems. In our practice, for example, we:
- focus on functional capacities, including the ability (or capacity) to understand language in meaningful contexts;
- work “top down” on expressive and receptive language tasks (not sub-skills and processes); and
- we try to work (or emulate) contexts that are helpful to a client in their real world (e.g. at home, school, work, in the community, and in social settings).
You can read more about our general approach to language therapy here.
Many other professionals (including many speech pathologists) take a more “bottom up” approach, working on processes and sub-skills, e.g. auditory processing, working memory, and executive functioning. This is based on a theory that gains in the efficiency of a process that underpins language will result in language and reading comprehension gains.
We try to keep an open mind about approaches that focus on sub-processes underpinning language because they are appealing in theory, and logical. But, to date, we’ve yet to see much independent, quality peer-reviewed evidence showing that improvements in specific sub-processes transfer to gains in language skills.
3. Why does oral language comprehension matter so much?
Good oral language comprehension skills help people to survive and thrive across their lifespan, including:
- as babies and toddlers learning to speak, and to understand, and to say their first words;
- as preschoolers, e.g. when learning language with their parents, peers and educators, e.g. through play, books and audiobooks;
- as young students starting school, e.g., with school readiness;
- as students at school, including understanding words, understanding complex grammar, following instructions, and understanding verbal maths problems and other STEM subjects;
- as readers of all ages;
- as high schoolers, e.g. with school success, generally, including understanding Tier 2 and academic vocabulary;
- with appropriate texting and social media use;
- with higher level study and lifelong learning skills;
- in the workforce, including understanding legal rights and responsibilities, following reasonable directions, and dealing with conflicts;
- understanding their consumer rights and responsibilities;
- with financial literacy;
- interacting with the government authorities, including the justice system;
- not being exploited or scammed, e.g. by misleading claims, charlatans, scammers, conspiracy theories, and schemes;
- enjoying many hobbies and interests;
- having healthy relationships with family members, romantic partners, and friendships;
- staying healthy and fit and understanding your rights to your health information;
- retirement; and
- old age.
4. How do we test oral language comprehension?
Lots of norm-referenced and criterion-referenced tests claim to measure oral language comprehension. It’s important to test different components of oral language:
- Oral comprehension of words is often assessed by showing people multiple pictures and asking them to point to the item(s) you name or describe. For example, you might ask a young person to look at these pictures:




“Point to the duck” or “Point to the bird with the long neck” or “Point to the ones with feathers” or “Point to the one that cannot fly” or “Point to the one that lives on a farm” or “Point to the one with a cockpit”.
- Oral language comprehension of complex and multi-part instructions is often assessed by giving the person instructions and asking them to do what you say. For example, you might show them these pictures:



Then, you would say something like:
“Before you point to the red star, point to the white triangle and the yellow circle” or “If the star is blue, point to the white triangle, but if the star is not blue point to the shape with no sides” or “Point to the one in the middle after pointing to the one on the left, and then point to the one that is between two other shapes”.
For younger clients, you might give them instructions using things nearby, e.g.: “Throw the bear, hug the ball, and then stand on the chair.” (We explain below why these instructions are so weird.)
- Oral comprehension of sentence structures (including morphology and complex sentences) is often tested by showing multiple pictures or videos and asking a person to point to the one you say. For example, to test comprehension of passive sentences, you might show the person these videos and then say:
“Point to ‘The TIE Fighter that is being chased by the dragon’.”
- We test referential and inferential oral comprehension of discourse by reading out paragraphs or stories (without showing the person the text) and then asking the person to answer questions about them. These often look like traditional comprehension exercises (but we read the passages out loud to the person being tested).
5. Oral language comprehension is hard to measure accurately
A person’s oral language comprehension is hard to test reliably for several reasons:
- We can’t truly know what is going on inside someone else’s head during a test.
- Lots of things can affect how a person performs on a language comprehension test. These include:
- background noise;
- attention;
- lack of sleep;
- sensorineural hearing issues, (including for people fitted with cochlear implants and hearing aids);
- conductive hearing difficulties;
- anxiety, depression, and other mental health issues;
- speech sound disorders;
- stuttering and other speech fluency disorders;
- expressive language problems;
- education and socio-economic factors, and home literacy environment;
- the person’s general health (e.g. chronic health conditions);
- for bilingual people, the language(s) used in the test (and the person’s language history);
- the test design, e.g. the sample size, validity and reliability of the test itself, and who was selected to work out the test norms and averages;
- the person’s level of comfort and rapport with the person testing them; and
- the person’s willingness to be tested!
- Most of us use sneaky tricks, e.g. adopting rules of thumb like “do what you normally do with a thing” when we don’t understand what someone has said to us. Tricks like these are the main reason we said “throw the bear and hug the ball” in our instruction example above (rather than the other way around, which would be more natural).
- In the real world, people rely on and and imitate others, even when we don’t understand why. It’s a key strategy we all use, e.g. when traveling to a new country where we don’t speak the local language. These tricks help us to fit in, but can make it look like we understand more than we actually do.
In practice, we want to monitor a person’s language comprehension over time in different situations and on different functional tasks, and not over interpret the results of a single test.
6. There are fewer effective treatments for receptive language difficulties (compared to expressive language interventions)
Most evidence-based language interventions to date target expressive language, rather than receptive language. There are many reasons for this:
- There is less evidence that receptive language interventions work (e.g. Law et al., 2003; and Rinaldi et al., 2021).
- Compared with people with expressive language difficulties, there are fewer clients with language comprehension problems (making it harder to recruit them for studies).
- In some cases, severe weaknesses in language comprehension are associated with weaker cognitive skills (even if they remain within normal limits overall), making treatment more challenging (e.g. Rinaldi et al., 2021).
- Compared with typically developing children and children with expressive language difficulties only, children with receptive language and “mixed” receptive-expressive language difficulties are more likely to have long-term issues with language development, literacy, behaviour and social development (e.g., Boyle et al., 2010).
- Some clinicians (including me) think the best way to improve receptive language skills (and to monitor comprehension) is to work on functional expressive language goals.
This is not to say there is no evidence to support language therapy for receptive language therapy. Here are some examples:
- in 2019, Dr Emily Dawes published a brilliant study that showed significant receptive language gains for a group of 5-year-old students’ comprehension of narratives and inferences. Very generously, Dr Dawes and her colleagues have published their treatment protocol and resources here. We use an adapted version of this intervention in our clinic with preschoolers and young students.
- In early 2022, Dr Acosta-Rodriguez and colleagues published a study outlining an effective intervention for referential and inferential oral language comprehension skills in preschoolers with developmental language disorder (see full citation below). The intervention involved a partnership between teachers and speech pathologists, and resulted in clinically significant improvements in understanding word classes, sentence structures, and semantic fluency; and
- In 2020, Tarvainen and colleagues published a study showing positive effects for oral language in students with developmental language disorder under 8 years of age.
Bottom line
We got there!
In this article, we outlined oral language comprehension as an idea, reviewed some models to help think about it in practice, and explained why it’s so important. We then looked at how oral language comprehension is assessed, and why it’s so hard to measure. We looked briefly at some of the evidence for helping people with language comprehension difficulties.
Let’s conclude by acknowledging we have a lot more to learn about language comprehension and language comprehension problems. We need more (and better) evidence-based programs to help people with difficulties understanding language, including for children, adolescents and adults with DLD and other language disorders.
Key source:
Acosta-Rodriguez, V.M., Ramírez-Santana, G.M. & Hernández-Expósito, S. (2022), Intervention for oral language comprehension skills in preschoolers with developmental language disorder. International Journal of Language and Communication Disorders. 57: 90-102. https://onlinelibrary.wiley.com/doi/full/10.1111/1460-6984.12676
*The distinction between spoken language and all noise is one of the main theoretical differences between oral language comprehension disorders and auditory processing disorders, although it’s confounded in practice by the fact that many auditory processing tests rely on or include language.
Related articles:
- Oral language: what is it and why does it matter so much for school, work, and life success?
- Language therapy works. But can we make it better? (October 2021 update, incorporating important research findings published in 2021)
- “I don’t understand what I’m reading” – reading comprehension problems (and what to do about them)
- Developmental Language Disorder (DLD): A free guide for families (2021) – revised and updated
- 24 practical ways to help school-aged children cope with language and reading problems at school and home
- How to help your school-age child learn new words – the nuts and bolts of how I actually do it in therapy
- Speaking for themselves: why I choose ambitious syntax goals to help students put their words together (with research updates and resource links)
- Following instructions: why so many of us struggle with more than one step
- For reading, school and life success, which words should we teach our kids? How should we do it?
- Focusing speech therapy on functional outcomes: a refresher
- Play-based, peer-mediated pragmatic language intervention for school-aged children
- Stories help students to understand and remember new information. Here’s why.
- Five ways to boost your child’s oral language and reading comprehension skills with sequencing
- Help your child to fill in the gaps, join the dots, and read between the lines! (Improve inferencing skills for better reading and language comprehension)
- What I think about when I meet a child who can’t read
- Too many children can’t read. We know what to do. But how should we do it?
- Dyslexia vs Developmental Language Disorder: same or different, and what do we need to know about their relationship?
- Not about ‘fixing’: using the ‘F-Word Framework’ to support children with communication disorders and their families
- Lockdown and oral language therapy: practical things we can do to make things better for everyone in these tough times
- Kick-start your child’s reading with speech sound knowledge (phonological awareness)
- When “steel meets steel”: grammar doesn’t need to be dull
- Parents: teach categories to your kids to ignite language development
- Light up language and reading comprehension with these key higher level language skills
- I want to help my late talker to speak, but I’m stuck at home. What can I do?
- Reading with – not to – your pre-schoolers: how to do it better (and why)
- Classic Audiobooks for Preschoolers
- Is your child ready for school? Focusing on what matters most
- My child used to be so good at maths. What happened?
- Starting high school? 6 practical, evidence-based principles to help students succeed at STEM subjects
- How to help our secondary teachers support teenagers with language disorders at school
- Want better school results? Avoid the hype and use free, evidence-based learning strategies
- Test Scores: What do they mean?
- My child is learning two languages: what do I need to know about bilingual development?
- Secret plans and clever tricks: how young children can fool us into thinking they understand more than they really do

Hi there, I’m David Kinnane.
Principal Speech Pathologist, Banter Speech & Language
Our talented team of certified practising speech pathologists provide unhurried, personalised and evidence-based speech pathology care to children and adults in the Inner West of Sydney and beyond, both in our clinic and via telehealth.
{kind=link}
Leave a Reply